Two posts ago, we made the rounds of the commonly measured blood lipids (total cholesterol, LDL, HDL, triglycerides) and how they associate with cardiac risk. It's important to keep in mind that many things associate with cardiac risk, not just blood lipids. For example, men with low serum vitamin D are at a 2.4-fold greater risk of heart attack than men with higher D levels. That alone is roughly equivalent to the predictive power of the blood lipids you get measured at the doctor's office. Coronary calcium scans (a measure of blood vessel calcification) also associate with cardiac risk better than the most commonly measured blood lipids.
Lipoproteins Can be Subdivided into Several Subcategories
In the continual search for better measures of cardiac risk, researchers in the 1980s decided to break down lipoprotein particles into sub-categories. One of these researchers is Dr. Ronald M. Krauss. Krauss published extensively on the association between lipoprotein size and cardiac risk, eventually concluding (source): The plasma lipoprotein profile accompanying a preponderance of small, dense LDL particles (specifically LDL-III) is associated with up to a threefold increase in the susceptibility of developing [coronary artery disease]. This has been demonstrated in case-control studies of myocardial infarction and angiographically documented coronary disease.
Krauss found that small, dense LDL (sdLDL) doesn't travel alone: it typically comes along with low HDL and high triglycerides*. He called this combination of factors "lipoprotein pattern B"; its opposite is "lipoprotein pattern A": large, buoyant LDL, high HDL and low triglycerides. Incidentally, low HDL and high triglycerides are hallmarks of the metabolic syndrome, the quintessential modern metabolic disorder.
Krauss and his colleagues went on to hypothesize that sdLDL promotes atherosclerosis because of its ability to penetrate the artery wall more easily than large LDL. He and others subsequently showed that sdLDL are also more prone to oxidation than large LDL (1, 2).
Diet Affects LDL Subcategories
The next step in Krauss's research was to see how diet affects lipoprotein patterns. In 1994, he published a study comparing the effects of a low-fat (24%), high-carbohydrate (56%) diet to a "high-fat" (46%), "low-carbohydrate" (34%) diet on lipoprotein patterns. The high-fat diet also happened to be high in saturated fat-- 18% of calories. He found that (quote source): Out of the 87 men with pattern A on the high-fat diet, 36 converted to pattern B on the low-fat diet... Taken together, these results indicate that in the majority of men, the reduction in LDL cholesterol seen on a low-fat, high-carbohydrate diet is mainly because of a shift from larger, more cholesterol-enriched LDL to smaller, cholesterol-depleted LDL [sdLDL].
In other words, in the majority of people, high-carbohydrate diets lower LDL cholesterol not by decreasing LDL particle count (which might be good), but by decreasing LDL size and increasing sdLDL (probably not good). This has been shown repeatedly, including with a 10% fat diet and in children. However, in people who already exhibit pattern B, reducing fat does reduce LDL particle number. Keep in mind that the majority of carbohydrate in modern America comes from wheat and sugar.
Krauss then specifically explored the effect of saturated fat on LDL size (free full text). He re-analyzed the data from the study above, and found that: In summary, the present study showed that changes in dietary saturated fat are associated with changes in LDL subclasses in healthy men. An increase in saturated fat, and in particular, myristic acid [as well as palmitic acid], was associated with increases in larger LDL particles (and decreases in smaller LDL particles). LDL particle diameter and peak flotation rate [density] were also positively associated with saturated fat, indicating shifts in LDL-particle distribution toward larger, cholesterol-enriched LDL.
Participants who ate the most saturated fat had the largest LDL, and vice versa. Kudos to Dr. Krauss for publishing these provocative data. It's not an isolated finding. He noted in 1994 that: Cross-sectional population analyses have suggested an association between reduced LDL particle size and relatively reduced dietary animal-fat intake, and increased consumption of carbohydrates.
Diet Affects HDL Subcategories
Krauss also tested the effect of his dietary intervention on HDL. Several studies have found that the largest HDL particles, HDL2b, associate most strongly with HDL's protective effects (more HDL2b = fewer heart attacks). Compared to the diet high in total fat and saturated fat, the low-fat diet decreased HDL2b significantly. A separate study found that the effect persists at one year. Berglund et al. independently confirmed the finding using the low-fat American Heart Association diet in men and women of diverse racial backgrounds. Here's what they had to say about it:
The results indicate that dietary changes suggested to be prudent for a large segment of the population will primarily affect [i.e., reduce] the concentrations of the most prominent antiatherogenic [anti-heart attack] HDL subpopulation.
Saturated and omega-3 fats selectively increase large HDL. Dr. B. G. of Animal Pharm has written about this a number of times.
Wrapping it Up
Contrary to the simplistic idea that saturated fat increases LDL and thus cardiac risk, total fat and saturated fat have a complex influence on blood lipids, the net effect of which is unclear, but is associated with a lower risk of heart attacks. These blood lipid changes persist for at least one year, so they may represent a long-term effect. It's important to remember that the primary sources of carbohydrate in the modern Western diet are wheat and sugar. Are the blood lipid patterns that associate with heart attack risk in Western countries partially acting as markers of wheat and sugar intake?
* This is why you may read that small, dense LDL is not an "independent predictor" of heart attack risk. Since it travels along with a particular pattern of HDL and triglycerides, in most studies it does not give information on cardiac risk beyond what you can get by measuring other lipoproteins.
The Multiple Risk Factor Intervention trial was a very large controlled diet trial conducted in the 1980s. It involved an initial phase in which investigators screened over 350,000 men age 35-57 for cardiovascular risk factors including total blood cholesterol. 12,866 participants with major cardiovascular risk factors were selected for the diet intervention trial, while the rest were followed for six years. I discussed the intervention trial here.During the six years of the observational arm of MRFIT, investigators kept track of deaths in the patients they had screened. They compared the occurrence of deaths from multiple causes to the blood cholesterol values they had measured at the beginning of the study. Here's a graph of the results (source): Click on the graph for a larger image. Coronary heart disease does indeed rise with increasing total cholesterol in American men of this age group. But total mortality is nearly as high at low cholesterol levels as at high cholesterol levels. What accounts for the increase in mortality at low cholesterol levels, if not coronary heart disease? Stroke is part of the explanation. It was twice as prevalent in the lowest-cholesterol group as it was in other participants. But that hardly explains the large increase in mortality. Possible explanations from other studies include higher cancer rates and higher rates of accidents and suicide. But the study didn't provide those statistics so I'm only guessing.The MRFIT study cannot be replicated, because it was conducted at a time when fewer people were taking cholesterol-lowering drugs. In 2009, a 50-year old whose doctor discovers he has high cholesterol will likely be prescribed a statin, after which he will probably no longer have high cholesterol. This will confound studies examining the association between blood cholesterol and disease outcomes.
Click on the graph for a larger image. Coronary heart disease does indeed rise with increasing total cholesterol in American men of this age group. But total mortality is nearly as high at low cholesterol levels as at high cholesterol levels. What accounts for the increase in mortality at low cholesterol levels, if not coronary heart disease? Stroke is part of the explanation. It was twice as prevalent in the lowest-cholesterol group as it was in other participants. But that hardly explains the large increase in mortality. Possible explanations from other studies include higher cancer rates and higher rates of accidents and suicide. But the study didn't provide those statistics so I'm only guessing.The MRFIT study cannot be replicated, because it was conducted at a time when fewer people were taking cholesterol-lowering drugs. In 2009, a 50-year old whose doctor discovers he has high cholesterol will likely be prescribed a statin, after which he will probably no longer have high cholesterol. This will confound studies examining the association between blood cholesterol and disease outcomes.
Thanks to The Great Cholesterol Con by Anthony Colpo for the MRFIT reference.
Now that we've seen that the first half of the diet-heart hypothesis-- that dietary saturated fat and cholesterol elevate serum cholesterol and low-density lipoprotein (LDL)-- is false, let's take a look at the second half. This is the idea that elevated serum cholesterol causes cardiovascular disease, also called the "lipid hypothesis".
Heart Attack Mortality vs. Total Mortality
We've been sternly warned that high serum cholesterol leads to heart attacks and that it should be reduced by any means necessary, including powerful cholesterol-lowering drugs. We've been assailed by scientific articles and media reports showing associations between cholesterol and heart disease. What I'm going to show you is a single graph that puts this whole issue into perspective.
The following is drawn from the Framingham Heart study (via the book Prevention of Coronary Heart Disease, by Dr. Harumi Okuyama et al.), which is one of the longest-running observational studies ever conducted. The study subjects are fairly representative of the general population, although less racially diverse (largely Caucasian). The graph is of total mortality (vertical axis) by total cholesterol level (horizontal axis), for different age groups: 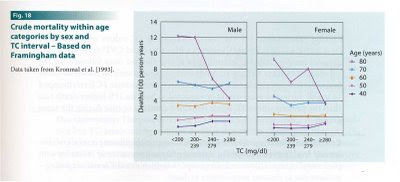 If you're 80 or older, and you have low cholesterol, it's time to get your affairs in order. Between the age of 50 and 80, when most heart attacks occur, there's no association between cholesterol level and total mortality. At age 50 and below, men with higher cholesterol die more often. In the youngest age group, the percent increase in mortality between low and high cholesterol is fairly large, but the absolute risk of death at that age is still low. There is no positive association between total cholesterol and mortality in women at any age, only a negative association in the oldest age group.
If you're 80 or older, and you have low cholesterol, it's time to get your affairs in order. Between the age of 50 and 80, when most heart attacks occur, there's no association between cholesterol level and total mortality. At age 50 and below, men with higher cholesterol die more often. In the youngest age group, the percent increase in mortality between low and high cholesterol is fairly large, but the absolute risk of death at that age is still low. There is no positive association between total cholesterol and mortality in women at any age, only a negative association in the oldest age group.
Here's more data from the Framingham study, this time heart attack deaths rather than total mortality (from the book Prevention of Coronary Heart Disease, by Dr. Harumi Okuyama et al.):  Up to age 47, men with higher cholesterol have more heart attacks. At ages above 47, cholesterol does not associate with heart attacks or total mortality. Since the frequency of heart attacks and total mortality are low before the age of 47, it follows that total cholesterol isn't a great predictor of heart attacks in the general population.
Up to age 47, men with higher cholesterol have more heart attacks. At ages above 47, cholesterol does not associate with heart attacks or total mortality. Since the frequency of heart attacks and total mortality are low before the age of 47, it follows that total cholesterol isn't a great predictor of heart attacks in the general population.
These findings are consistent with other studies that looked at the relationship between total cholesterol and heart attacks in Western populations. For example, the observational arm of the massive MRFIT study found that higher cholesterol predicted a higher risk of heart attack in men age 35-57, but total mortality was highest both at low and high cholesterol levels. The "ideal" cholesterol range for total mortality was between 140 and 260 mg/dL (reference). Quite a range. That encompasses the large majority of the American public.
The Association Between Blood Cholesterol and Heart Attacks is Not Universal
The association between total cholesterol and heart attacks has generally not been observed in Japanese studies that did not pre-select for participants with cardiovascular risk factors (Prevention of Coronary Heart Disease, by Dr. Harumi Okuyama et al.). They also aren't observed on Kitava, where no one seems to have heart attacks or stroke regardless of cholesterol. This suggests that total blood cholesterol as a marker of heart attack risk is not universal. I suspect it would not necessarily apply to someone eating an atypical diet.
Subdividing Cholesterol into Different Lipoprotein Particles Improves its Predictive Value
So far, this probably hasn't shocked anyone. Even entrenched proponents of the lipid hypothesis admit that total cholesterol isn't a great marker. Researchers long ago sliced up total cholesterol into several more specific categories, the most discussed being low-density lipoprotein (LDL) and high-density lipoprotein (HDL). These are tiny fatty droplets containing fats, cholesterol and proteins. They transport cholesterol, fats, and fat-soluble vitamins between tissues via the blood.
The LDL and HDL numbers you get back from the doctor's office typically refer to the amount of cholesterol contained in LDL or HDL per unit blood serum, but you can get the actual particle number measured as well. One can also measure the level of triglyceride (a type of fat) in the blood. Triglycerides are absorbed from the digestive tract and manufactured by the liver in response to carbohydrate, then sent to other organs via lipoproteins.
The level of LDL in the blood gives a better approximation of heart attack risk than total cholesterol. If you're living the average Western lifestyle and you have high LDL, your risk of heart attack is up to twice the risk of someone who has low LDL. LDL particle number has more predictive value than LDL cholesterol concentration. The latter is what's typically measured at the doctor's office. For example, in the EPIC-Norfolk study (free full text), patients with high LDL cholesterol concentration had a 73% higher risk of heart attack than patients with low LDL. Participants with high LDL particle number had exactly twice the risk of those with low LDL number. We'll get back to this phenomenon in a future post.
In the same study, participants with low HDL had twice the heart attack risk of participants with high HDL. That's why HDL is called "good cholesterol". This finding is fairly consistent throughout the medical literature. HDL is probably the main reason why total cholesterol doesn't associate very tightly with heart attack risk. High total cholesterol doesn't tell you if you have high LDL, high HDL or both (LDL and HDL are the predominant cholesterol-carrying lipoproteins). Also from the EPIC-Norfolk study, participants with high triglycerides had twice the risk of heart attack as participants with low triglycerides. Triglycerides and HDL are inversely related to one another, that is, if a person has high HDL, they're likely to have low triglycerides, and vice versa. This has also been consistent between studies.
Together, this suggests that the commonly measured lipoprotein pattern that associates most tightly with heart attack risk in typical Western populations is high LDL (particularly LDL particle number), low HDL and high triglycerides.
In the next post, I'll slice up the lipoproteins even further and comment on their association with cardiovascular disease. I'll also begin to delve into how diet affects the lipoproteins.
The diet-heart hypothesis is the idea that (1) dietary saturated fat, and in some versions, dietary cholesterol, raise blood cholesterol in humans and (2) therefore contribute to the risk of heart attack.
I'm not going to spend a lot of time on the theory in relation to dietary cholesterol because there really isn't much evidence to debunk in humans. As far as I can tell, most diet-health researchers don't take this theory seriously anymore because the evidence has simply failed to materialize. Dr. Walter Willett doesn't believe it, and even Dr. Ancel Keys didn't believe it. Here's a graph from the Framingham Heart study (via the book Prevention of Coronary Heart Disease, by Dr. Harumi Okuyama et al.) to drive home the point. Eggs are the most concentrated source of cholesterol in the American diet. In this graph, the "low" group ate 0-2 eggs per week, the "medium" group ate 3-7, and the "high" group ate 7-14 (click for larger image): 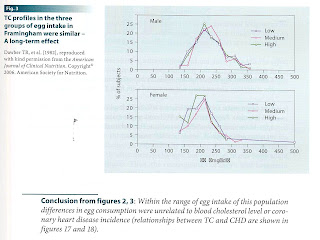 The distribution of blood cholesterol levels between the three groups was virtually identical. The study also found no association between egg consumption and heart attack risk. Dietary cholesterol does not raise serum cholesterol in the long term, because humans are adapted to eating cholesterol. We simply adjust our own cholesterol metabolism to compensate when the amount in the diet increases, like dogs. Rabbits don't have that feedback mechanism because their natural diet doesn't include cholesterol, so feeding them dietary cholesterol increases blood cholesterol and causes vascular pathology.
The distribution of blood cholesterol levels between the three groups was virtually identical. The study also found no association between egg consumption and heart attack risk. Dietary cholesterol does not raise serum cholesterol in the long term, because humans are adapted to eating cholesterol. We simply adjust our own cholesterol metabolism to compensate when the amount in the diet increases, like dogs. Rabbits don't have that feedback mechanism because their natural diet doesn't include cholesterol, so feeding them dietary cholesterol increases blood cholesterol and causes vascular pathology.
The first half of the diet-heart hypothesis states that eating saturated fat raises blood cholesterol. This has been accepted without much challenge by mainstream diet-health authorities for nearly half a century. In 1957, Dr. Ancel Keys proposed a formula (Lancet 2:1959. 1957) to predict changes in total cholesterol based on the amount of saturated and polyunsaturated fat in the diet. This formula, based primarily on short-term trials from the 1950s, stated that saturated fat is the primary dietary influence on blood cholesterol.
According to Keys' interpretation of the trials, saturated fat raised, and to a lesser extent polyunsaturated fat lowered, blood cholesterol. But there were serious flaws in the data from the very beginning, which were pointed out in this searing 1973 literature review in the American Journal of Clinical Nutrition (free full text).
The main problem is that the controlled trials typically compared saturated fats to omega-6 linoleic acid (LA)-rich vegetable oils, and when serum cholesterol was higher in the saturated fat group, this was most often attributed to the saturated fat raising blood cholesterol rather than the LA lowering it. When a diet high in saturated fat was compared to the basal diet without changing LA, often no significant increase in blood cholesterol was observed. Studies claiming to show a cholesterol-raising effect of saturated fat often introduced it after an induction period rich in LA. Thus, the effect may have more to do with LA lowering blood cholesterol than saturated fat raising it. This is not at all what I was expecting to find when I began looking through the short-term trials.I recently read a 2003 study that addresses this point directly. Muller et al. (free full text) compared the effects of three controlled diets on the blood cholesterol of 25 healthy women. The diets were: - High in saturated fat from coconut, low in LA
- Same as #1, with half the saturated fat replaced by carbohydrate
- Low in saturated fat, high in LA, with the same total fat as in #1
The diets were fed to the whole group for three week periods. Investigators found that diet #3 lowered cholesterol and LDL relative to diets #1 and #2. The total cholesterol of women on diets #1 and #2 were not statistically different (p= 0.09), and their LDL was virtually identical. Thus, a very large difference in saturated fat intake didn't affect total cholesterol or LDL when it was replaced by carbohydrate, but it did when it was replaced by LA. The most straightforward explanation is that LA lowers cholesterol and LDL, but saturated fat has little or no effect on either. From the discussion section:
The most important finding of this study was that lowering total saturated fat in the form of coconut oil, from 22.7 to 10.5 E% without change in the P/S ratio [polyunsaturated to saturated ratio], did not lower total or LDL cholesterol, but significantly reduced HDL cholesterol.
I don't claim that this one study settles the question, but does illustrate that saturated fat does not have a large and consistently detectable effect on total or LDL cholesterol. Among the many other studies I examined, I found an apparently well-controlled counterexample: Arterioscler. Thromb. Vasc. Biol. 18:441. 1988. In this 8-week study, increasing saturated fat (at the expense of carbohydrate and with LA constant) increased total cholesterol and LDL, while also increasing HDL, and decreasing Lp(a) and triglycerides (the latter three changes are thought to be protective). Decreasing saturated fat from 15% to 6% of calories (drastic), reduced total cholesterol by 9% and LDL by 11% (calculated by the Friedewald equation). The variation between trials may have to do with the specific saturated fatty acids used in each trial, their duration, or some other unknown confounder.
Reading through the short-term controlled trials, I was struck by the variability and lack of agreement between them. Some of this was probably due to a lack of control over variables and non-optimal study design. But if saturated fat has a dominant effect on serum cholesterol in the short term, it should be readily and consistently demonstrable. It clearly is not.The long-term data are also not kind to the diet-heart hypothesis. Reducing saturated fat while greatly increasing LA certainly does lower blood cholesterol substantially. This was the finding in the well-controlled Minnesota Coronary Survey trial, for example (14% reduction). But in other cases where LA intake changed less, such as MRFIT, the Women's Health Initiative Diet Modification trial and the Lyon Diet-Heart trial, reducing saturated fat intake had little or no effect on total cholesterol or LDL (0-3% reduction). This generally dumbfounded the investigators. The small changes that did occur could easily have been due to other factors, such as increased fiber and phytosterols, since these were multiple-factor interventions.
Another blow to the idea that saturated fat raises cholesterol in the long term comes from observational studies. Here's a graph of data from the Health Professionals Follow-up study, which followed 43,757 health professionals for 6 years (via the book Prevention of Coronary Heart Disease by Dr. Harumi Okuyama et al.):  What this graph shows is that at a relatively constant LA intake, neither saturated fat intake nor the ratio of LA to saturated fat were related to blood cholesterol in freely living subjects. This was true across a wide range of saturated fat intakes (7-15%). If we can't even find a consistent association between dietary saturated fat and blood cholesterol in observational studies, how can we claim that saturated fat is a dominant influence on blood cholesterol?
What this graph shows is that at a relatively constant LA intake, neither saturated fat intake nor the ratio of LA to saturated fat were related to blood cholesterol in freely living subjects. This was true across a wide range of saturated fat intakes (7-15%). If we can't even find a consistent association between dietary saturated fat and blood cholesterol in observational studies, how can we claim that saturated fat is a dominant influence on blood cholesterol?
There's more. If saturated fat were important in determining the amount of blood cholesterol in the long term, you'd expect populations who eat the most saturated fat to have high blood cholesterol levels. But that's not at all the case. The Masai traditionally get almost 2/3 of their calories from milk fat, half of which is saturated. In 1964, Dr. George V. Mann published a paper showing that traditional Masai warriors eating nothing but very fatty milk, blood and meat had an average cholesterol of 115 mg/dL in the 20-24 year age group. For comparison, he published values for American men in the same age range: 198 mg/dL (J. Atherosclerosis Res. 4:289. 1964). Apparently, eating three times the saturated animal fat and several times the cholesterol of the average American wasn't enough to elevate their blood cholesterol. What does elevate the cholesterol of a Masai man? Junk food.
Now let's swim over to the island of Tokelau, where the traditional diet includes nearly 50% of calories from saturated fat from coconut. This is the highest saturated fat intake of any population I'm aware of. How's their cholesterol? Men in the age group 20-24 had a concentration of 168 mg/dL in 1976, which was lower than Americans in the same age group despite a four-fold higher saturated fat intake. Tokelauans who migrated to New Zealand, eating half the saturated fat of their island relatives, had a total cholesterol of 191 mg/dL in the same age group and time period, and substantially higher LDL (J. Chron. Dis. 34:45. 1981). Sucrose consumption was 2% on Tokelau and 13% in New Zealand. Saturated fat seems to take a backseat to some other diet/lifestyle factor(s). Body fatness and excess calorie intake are good candidates, since they influence circulating lipoproteins.
I have to conclude that if saturated fat influences total cholesterol or LDL concentration at all, the effect is modest and is secondary to other factors.
The other day, my internet meanderings brought me back to a review of fat modification trials conducted by the Cochrane collaboration. This is a not-for-profit group known for its rigorous meta-analyses.
They selected 27 studies that reduced saturated fat or total fat (in some cases along with increased PUFA), and fit several inclusion criteria. The results: There was no significant effect on total mortality (rate ratio 0.98, 95% CI 0.86 to 1.12), a trend towards protection form cardiovascular mortality (rate ratio 0.91, 95% CI 0.77 to 1.07), and significant protection from cardiovascular events (rate ratio 0.84, 95% CI 0.72 to 0.99). The latter became non-significant on sensitivity analysis.
Trials where participants were involved for more than 2 years showed significant reductions in the rate of cardiovascular events and a suggestion of protection from total mortality ["suggestion" = not statistically significant]. The degree of protection from cardiovascular events appeared similar in high and low risk groups, but was statistically significant only in the former.
"Sensitivity analysis" is a statistical method that allows investigators to take into account the limitations of their model, in this case, the way in which they aggregated the studies' data. Another way of putting their findings is that they found no significant effect of fat modification on mortality or cardiovascular mortality, and they found a reduction in non-fatal "cardiovascular events" (more on this phrase later) only in a subset of the data.
I'll be the first to admit the meta-analysis isn't perfect. They cast too wide a net, not allowing them to distinguish the effect of reducing total fat from the effect of reducing saturated fat. They lumped both together, which from a practical standpoint isn't actually a problem because both sets of studies show essentially the same thing: zilch. But it's still not the best way to conduct a meta-analysis. They also omitted the Sydney Diet-Heart study for mysterious reasons, which was a five year randomized trial that found an increase in mortality in volunteers substituting vegetable oils for animal fat. Then there's the conclusion, which boggles the mind: Lifestyle advice to all those at high risk of cardiovascular disease (especially where statins are unavailable or rationed), and to lower risk population groups, should continue to include permanent reduction of dietary saturated fat and partial replacement by unsaturates.
Are these the same people who wrote the results section? I don't understand how they arrived at that conclusion from their own results.
In any case, this brings me to my main point. There are two types of outcomes you can measure in these trials: "hard endpoints" and "soft endpoints". Hard endpoints are not subjective. The hardest endpoint is death. Either you're dead or you aren't; there's no room for interpretation there. A bit less hard is death from a particular cause, such as heart attack. In that case, you're definitely dead, but the physician has to guess what you died of. That involves some judgment on the part of the physician and can introduce bias, depending on the study design. The softest endpoints are non-fatal events like angina, bypasses and stents. These depend on the judgment of both the physician and the patient, and are the most susceptible to bias.
The gold standard for controlled trials is a design known as "double-blind", where neither the participant nor the physician knows which group the participant is in. This design eliminates bias from both the participant and the physician side, allowing correction for the placebo effect and subtle bias in diagnosis. This is easy to do for drug trials, where placebo pills look just like the drug. But it's more difficult to pull off in a diet trial, where the patient knows what foods he's eating. Still, it can be done by giving participants similar-looking margarines containing either saturated or polyunsaturated fats, or sometimes by controlling diets in an institutionalized setting.
There have been three double-blind trials comparing the incidence of heart attack and/or mortality in volunteers eating either saturated animal fat or polyunsaturated vegetable fat: the 1968 National Diet-Heart trial (2 years), the 1969 Los Angeles Veterans' Administration trial (8 years), and the 1989 Minnesota Coronary Survey trial (4.5 years). The two studies that reported total mortality found no significant difference between groups. Two out of three found no difference in heart attack deaths. Of the two that reported on non-fatal cardiovascular endpoints, one found a significant difference. The V.A. trial was the only one to find a significant difference in heart attack deaths (18% decrease) and non-fatal events. There were significantly more heavy smokers in the animal fat arm of the V.A. trial, which was an unfortunate consequence of the participant randomization process. So that result is difficult to interpret.
The three double-blind diet trials, with the least potential for bias, really give no support to the idea that saturated/animal fat contributes to cardiovascular disease. As the participants were already eating a diet high in omega-6 to begin with, there is also no detectable effect of increasing omega-6 on cardiovascular health.
Many of the trials of this nature have been "single-blinded", where the participant knows which group he's in, but the physician doesn't. In this case, all endpoints involving death will be unbiased, because the physician deciding the diagnosis is not influenced by knowing what group the patient is in. However, soft, non-fatal events such as angina are still highly susceptible to the placebo effect. This is because they depend on the subjective judgment of the patient, who knows which group he's in.
I think it's interesting to note that very few dietary fat modification trials have found reductions in total mortality, which is the hardest endpoint and the least susceptible to bias. This is reflected in the Cochrane collaboration's findings. However, a number of the non-blinded and single-blinded studies have found differences in non-fatal cardiovascular events, sometimes creating absurd results. For example, in the 1966 Anti-Coronary Club trial, participants in the vegetable oil group had a significant reduction in non-fatal cardiovascular events, but a massive increase in cardiovascular deaths and total mortality. The former result could result from a placebo effect, due to the non-blinded nature of the trial.
The fact that the Cochrane review found statistically significant benefits of fat modification in soft, non-fatal endpoints (for a portion of the data set), but not endpoints involving death, suggests to me that what we're seeing may actually be a placebo effect resulting from the fact that patients were not blinded in the majority of these trials.
The only "fat modification" intervention that consistently reduces total and cardiovascular mortality is omega-3 fat supplementation, ideally in combination with omega-6 restriction. This is supported by the results of the DART trial, the Lyon Diet-Heart trial, the ISIS trial and the the GISSI-prevenzione trial.
This diet trial was conducted between 1959 and 1971 in two psychiatric hospitals near Helsinki, Finland. One hospital served typical fare, including full-fat milk and butter, while the other served "filled milk", margarine and polyunsaturated vegetable oils. Filled milk has had its fat removed and replaced by an emulsion of vegetable oil. As a result, the diet of the patients in the latter hospital was low in saturated fat and cholesterol, and high in polyunsaturated fat compared to the former hospital. At the end of six years, the hospitals switched diets. This is known as a "crossover" design.The results were originally published in 1972 in the Lancet (ref), and a subset of the data were re-published in 1979 in the International Journal of Epidemiology (ref). They found that during the periods that patients were eating the diet low in saturated fat and cholesterol, and high in vegetable oil, male participants (but not females) had roughly half the incidence of heart attack deaths. There were no significant differences in total mortality in either men or women. The female data were omitted in the 1979 report.This study is often cited as support for the idea that saturated fat increases the risk of heart attack. The reason it's cited so often is it's one of a minority of trials that came to that conclusion. The only other controlled trial I'm aware of that replaced animal fat with polyunsaturated vegetable oil (without changing other variables at the same time) and found a statistically significant decrease in cardiovascular deaths was the Los Angeles Veterans' Administration study. However, there was no difference in total mortality, and there were significantly more heavy smokers in the control group. The difference in heart attack deaths in the V.A. trial was 18%, far less than the difference seen in the Finnish trial. I can cite three controlled trials that came to the opposite conclusion, that switching saturated fat for vegetable oil increases cardiovascular mortality and/or total mortality: the Anti-Coronary Club Trial (4 years), the Rose et al. corn oil trial (2 years), and the Sydney Diet-Heart trial (5 years). Other controlled trials found no difference in total mortality or heart attack mortality from this intervention, including the National Diet-Heart Study (2 years) and the Medical Research Council study (7 years). Thus, the Finnish trial is an outlier whose findings have never been replicated by better-conducted trials.I have three main bones to pick with the Finnish trial. The first two are pretty bad, but the third is simply fatal to its use as support for the idea that saturated fat contributes to cardiovascular risk: 1) A "crossover" study design is not an appropriate way to study a disease with a long incubation period. How do you know that the heart attacks you're observing came from the present diet and not the one the patients were eating for the six years before that? The Finnish trial was the only trial of its nature ever to use a crossover design. 2) The study wasn't blinded. When one wants to eliminate bias in diagnosis for these types of studies, one designs the study so that the physician doesn't know which group the patients came from. That way he can't influence the results, consciously or unconsciously. Obviously there was no way to blind the physicians in this study, because they knew what the patients in each hospital were eating. I think it's interesting that the only outcome not susceptible to diagnostic bias, total mortality, showed no significant changes in either men or women. 3) The Finnish Mental Hospital trial was not actually a controlled trial. In an editorial in the November 1972 issue of the Lancet, Drs. John Rivers and John Yudkin pointed out, among other things, that the amount of sugar varied by almost 50% between diet periods. In the December 30th issue, the lead author of the study responded:In view of the design of the experiment the variations in sugar intake were, of course, regrettable. They were due to the fact that, aside from the fatty-acid composition and the cholesterol content of the diets, the hospitals, for practical reasons, had to be granted certain freedom in dietary matters.
In other words, the diets of the two hospitals differed significantly in ways other than their fat composition. Sugar was one difference. Carbohydrate intake varied by as much as 17% and total fat intake by as much as 26% between diet periods (on average, carbohydrate was lower and total fat was higher in the polyunsaturated fat group). The definition of a controlled trial is an experiment in which all variables are kept constant except the one being evaluated. Therefore, the Finnish trial cannot rightfully be called a controlled trial. This places it in the same category as other observational studies, in which variables are not controlled and one can only guess what factors caused the difference in disease incidence. The fact that the result has never been replicated casts further doubt on the study.
I could continue listing other problems with the study, such as the fact that the hospital population included in the analysis had a high turnover rate (variable, but as high as 40%), and patients were included in the analysis even if they were at the hospital for as little as 50% of the time between first admission and final discharge (i.e., they came and went). But what's the use in beating a dead horse?
The Finnish trial is still very useful, however. I use it as a litmus test to determine which papers are solid and which are desperate for data that confirm their biases. Any author who cites the Finnish trial in support of the idea that saturated fat causes heart attacks either isn't familiar with it, or is not objective.
 PART II: Milk and the Nature of Things: Gender, Race, Class, Species
PART II: Milk and the Nature of Things: Gender, Race, Class, Species
“The concealment of breastfeeding rests equally, if not more, on squeamishness relating to bodily function: the fact that food comes out of our bodies is an unsettling thought in a culture that rarely remembers food growing on trees”
--Fiona Giles Fresh Milk [*]
“Separate lexicons suggest opposite behaviors and attributes. We eat, but other animals feed. A woman is pregnant or nurses her babies; a nonhuman mammal gestates or lactates. A dead human is a corpse, a dead nonhuman a carcass or meat”
--Carol Adams “Foreword” to Animal Equality[*]
"[W]ithin Linnaeus terminology [Homo sapien], a female characteristic (the lactating mamma) ties humans to brutes, while a traditionally male characteristic (reason) marks our separation”
--Londa Shiebinger "Why Mammals are Called Mammals"[*]
Just as breasts (generally) come in pairs, so do their culturally conscripted “natures.” Londa Shiebinger writes:the female breast ha[s] been a powerful icon within Western cultures, representing both the sublime and bestial in human nature. The grotesque, withered breasts on witches and devils represented temptations of wanton lust, sin of the flesh, and humanity fallen from paradise. The firm spherical breasts of Aphrodite, the Greek ideal, represented an overworldly beauty and virginity.[51d]
As we saw in parts one and two, female breasts may represent all that which is most beautiful and divine to humans (i.e. the virgin mother of God) while any digression from their use to titillate males (i.e. lesbian sensuality) or nurture the young (i.e. sexual feelings while nursing) may represent all that is wrong with the world.
I will argue here in section two that the function of the human breast acts as a particularly sensitive subject because it is a site that may not only contest gender identities but that which may also contest modern “white” men’s proximity to “the animal.” Just as gynecomastia, male breast cancer, and male lactation challenge presuppositions about male identity, so does the very biological function of human breasts. As Shiebinger notes, "that breasts have "long been considered less than human, yet simultaneously "more than human."[51f]Read more »
There's a definite association between the consumption of refined carbohydrates and dental cavities. Dr. Weston Price pointed this out in a number of transitioning societies in his epic work Nutrition and Physical Degeneration. Many other anthropologists and dentists have observed the same thing.I believe, based on a large body of anthropological and medical data, that it's not just an association-- sugar and flour cause cavities. But why? Is it that they lack micronutrients-- the explanation favored by Price-- or do they harm teeth by feeding the bacteria that participate in cavity formation? Or both?I recently found an interesting article when I was perusing an old copy of the Journal of Dental Research: "A Comparison of Crude and Refined Sugar and Cereals in Their Ability to Produce in vitro Decalcification of Teeth", published in 1937 by Dr. T. W. B. Osborn et al. (free full text). I love old papers. They're so free of preconceptions, and they ask big questions. The authors begin with the observation that the South African Bantu, similar to certain cultures Dr. Price visited, had a low prevalence of tooth decay when eating their native diet high in unrefined carbohydrate foods. However, their decay rate increased rapidly as modern foods such as white flour and refined sugar became available. To test whether refined carbohydrates have a unique ability to cause tooth decay, the investigators took pieces of teeth that had been extracted for reasons other than decay (for example, crowding), and incubated them with a mixture of human saliva and several different carbohydrate foods:- crude cane juice
- refined cane sugar
- whole wheat flour
- white wheat flour
- whole corn meal
- refined corn meal
After incubating teeth in the solutions for 2-8 weeks at 37 C (human body temperature), they had trained dentists evaluate them for signs of decalcification. Decalcification is a loss of minerals that is part of the process of tooth decay. Teeth, like bones, are mineralized primarily with calcium and phosphorus, and there is a dynamic equilibrium between minerals leaching out of the teeth and minerals entering them.The researchers used teeth incubated in saline solution as the reference. The dentists were "blinded", meaning they didn't know which solution each tooth came from. This is a method of reducing bias. Here are some of the results. Cane juice vs. refined sugar: Unrefined cane juice was not very effective at causing decalcification, compared to refined sugar. This was a surprise to me. Here is the result for wheat:
Unrefined cane juice was not very effective at causing decalcification, compared to refined sugar. This was a surprise to me. Here is the result for wheat: Note that the scale is different on this graph. Wheat, and particularly refined wheat, is very good at decalcifying teeth in vitro. Corn:
Note that the scale is different on this graph. Wheat, and particularly refined wheat, is very good at decalcifying teeth in vitro. Corn: Refined corn is much more effective at decalcifying teeth than whole meal corn. Next, the investigators performed an experiment where they compared the three types of refined carbohydrate to one another:
Refined corn is much more effective at decalcifying teeth than whole meal corn. Next, the investigators performed an experiment where they compared the three types of refined carbohydrate to one another:  As one would predict from the graphs above, refined wheat is worse than refined corn, is worse than refined sugar. This is really at odds with conventional wisdom. It's important to keep in mind that these results are not necessarily directly applicable to a living human being, who wouldn't let a mouthful of wheat porridge sit in his mouth for five weeks. But it does show that refining carbohydrates may increase their ability to cause cavities due to a direct effect on the teeth (rather than by affecting whole-body nutritional status, which they do as well).The authors tested the acidity of the different solutions, and found no consistent differences between them (they were all at pH 4-5 within 24 hours), so acid production by bacteria didn't account for the results. They speculated that the mineral content of the unrefined carbohydrates may have prevented the bacterial acids from leaching minerals out of the teeth. Fortunately for us, they went on to test that speculation in a series of further investigations. In another paper, Dr. T. W. B. Osborn and his group showed that they could greatly curb the decalcification process by adding organic calcium and phosphorus salts to the solution. This again points to a dynamic equilibrium, where minerals are constantly leaving and entering the tooth structure. The amounts of calcium and phosphorus required to inhibit calcification were similar to the amounts found in unrefined cane sugar, wheat and corn. This suggests the straightforward explanation that refined sugar and grains cause decay at least in part because most of the minerals are removed during the refining process. However, we're still left with the puzzling fact that wheat and corn flour decalcify teeth in vitro more effectively than cane juice. I suspect that has to do with the phytic acid content of the grains, which binds the minerals and makes them partially unavailable to diffusion into the teeth. Cane juice contains minerals, but no phytic acid, so it may have a higher mineral availability. This explanation may not be able to account for the fact that refined sugar was also less effective at decalcifying teeth than refined wheat and corn flour. Perhaps the residual phytic acid in the refined grains actually drew minerals out of the teeth? No, I'm not saying you can eat sugar with impunity if it's unrefined. There isn't a lot of research on the effects of refined vs. unrefined sugar, but I suspect too much sugar in any form isn't good. But this does suggest that refined carbohydrates may be particularly effective at promoting cavities, due to a direct demineralizing effect on teeth subsequent to bacterial acid production. It also supports Dr. Price's contention that a food's micronutrient content is the primary determinant of its effect on dental health.
As one would predict from the graphs above, refined wheat is worse than refined corn, is worse than refined sugar. This is really at odds with conventional wisdom. It's important to keep in mind that these results are not necessarily directly applicable to a living human being, who wouldn't let a mouthful of wheat porridge sit in his mouth for five weeks. But it does show that refining carbohydrates may increase their ability to cause cavities due to a direct effect on the teeth (rather than by affecting whole-body nutritional status, which they do as well).The authors tested the acidity of the different solutions, and found no consistent differences between them (they were all at pH 4-5 within 24 hours), so acid production by bacteria didn't account for the results. They speculated that the mineral content of the unrefined carbohydrates may have prevented the bacterial acids from leaching minerals out of the teeth. Fortunately for us, they went on to test that speculation in a series of further investigations. In another paper, Dr. T. W. B. Osborn and his group showed that they could greatly curb the decalcification process by adding organic calcium and phosphorus salts to the solution. This again points to a dynamic equilibrium, where minerals are constantly leaving and entering the tooth structure. The amounts of calcium and phosphorus required to inhibit calcification were similar to the amounts found in unrefined cane sugar, wheat and corn. This suggests the straightforward explanation that refined sugar and grains cause decay at least in part because most of the minerals are removed during the refining process. However, we're still left with the puzzling fact that wheat and corn flour decalcify teeth in vitro more effectively than cane juice. I suspect that has to do with the phytic acid content of the grains, which binds the minerals and makes them partially unavailable to diffusion into the teeth. Cane juice contains minerals, but no phytic acid, so it may have a higher mineral availability. This explanation may not be able to account for the fact that refined sugar was also less effective at decalcifying teeth than refined wheat and corn flour. Perhaps the residual phytic acid in the refined grains actually drew minerals out of the teeth? No, I'm not saying you can eat sugar with impunity if it's unrefined. There isn't a lot of research on the effects of refined vs. unrefined sugar, but I suspect too much sugar in any form isn't good. But this does suggest that refined carbohydrates may be particularly effective at promoting cavities, due to a direct demineralizing effect on teeth subsequent to bacterial acid production. It also supports Dr. Price's contention that a food's micronutrient content is the primary determinant of its effect on dental health.
Reversing Tooth Decay
Preventing Tooth Decay
Dental Anecdotes
 Is it to men that nature confided domestic cares? Has she given us breasts to feed our children?”
Is it to men that nature confided domestic cares? Has she given us breasts to feed our children?”
--Pierre-Gaspard Chaumette quoted in "Why Mammals are Called Mammals"[*]
Experience may tell you that producing milk and nursing youngsters is a job for the female mammal, not the male. But your experience is probably limited, and the potential of biology--and medical technology--is vast.
--Jared Diamond "Father's Milk"[*]
"For those who claim male lactation is "unnatural," I would have to ask: how natural is canned formula from Nestle' or pacifiers made from petrolium byproducts? If milk production in men were truly unnatural, it wouldn't exist.”
--Laura Shanley "Milkmen: Fathers who Breastfeed"[*]
3. Male Lactation: An Unnatural Act?
The identity politics of human breasts come to full fruition in the question of male nipples. As male children we are taught that girls have “boobs” and boys have “chests,’ but the question of male nipples cannot be evaded. For thousands of years breasts have been one of the most significant markers of one’s gender, and hence male breasts and their nipples pose an existential dilemma to those who identify as male. This has never been truer than within the present visual culture that fetishizes the (female) breast.
Take for example the reception of the 2006 Nickelodeon film Barnyard. While critics had diverse opinions on the film, nearly all their reviews shared one particular quip: the protagonist of the film, a steer, had utters. As one late reviewer ranted: Every single review whether by a critic or just your average John Q. Moviefone seems to be possessed by the urge to point out their extensive knowledge of bovine anatomy and remind the reader that male cattle do not, in fact, have udders.[22]
While filmgoers often suspend disbelief during films, especially animated features, the audiences could not suspend “the truth” about male anatomy. And, of course, there is also the double standard. Female pigs (who have ten or more nipples) and chickens (who don’t have any mammary glands) are often represented with a pair of giant breasts in cartoons yet male reviewers say nothing—they probably are not even conscious of these transgressions. The existence of DD breasts on a chicken somehow seem quite natural, but udders on a male, no! (But if male goats can grow udders, why not steers?)[*]Read more »










